Acute-on-chronic liver failure (ACLF) is a complex syndrome that developed in patients with chronic liver disease of various aetiologies characterized by the acute deterioration of liver function and high short-term mortality. To date, few global cohorts encompassing all aetiologies have been established to develop unified diagnostic criteria for ACLF. Different international consortia have proposed varying definitions of ACLF based on regional cohorts with specific aetiologies, resulting in considerable confusion regarding diagnosis and the application of management recommendations.
A research team led by Prof. Jun Li from the First Affiliated Hospital, Zhejiang University School of Medicine previously developed the Chinese Group on the Study of Severe Hepatitis B (COSSH) criteria, the China-CLIF score (formerly COSSH-ACLF score), and its simplified version, the COSSH-ACLF II score, which have been validated as suitable for hepatitis B virus (HBV)-related populations.
Building on this foundation, the team established the first prospective multicentre study cohort that included nearly all major ACLF aetiologies and collaborated with leading international cohorts. Their findings, recently published in Gut under the title “Performance of the China-CLIF framework in acute-on-chronic liver failure: a multicohort study across all aetiologies”, demonstrate that the China-CLIF framework offers broader applicability across diverse aetiologies and geographic regions compared with existing systems.
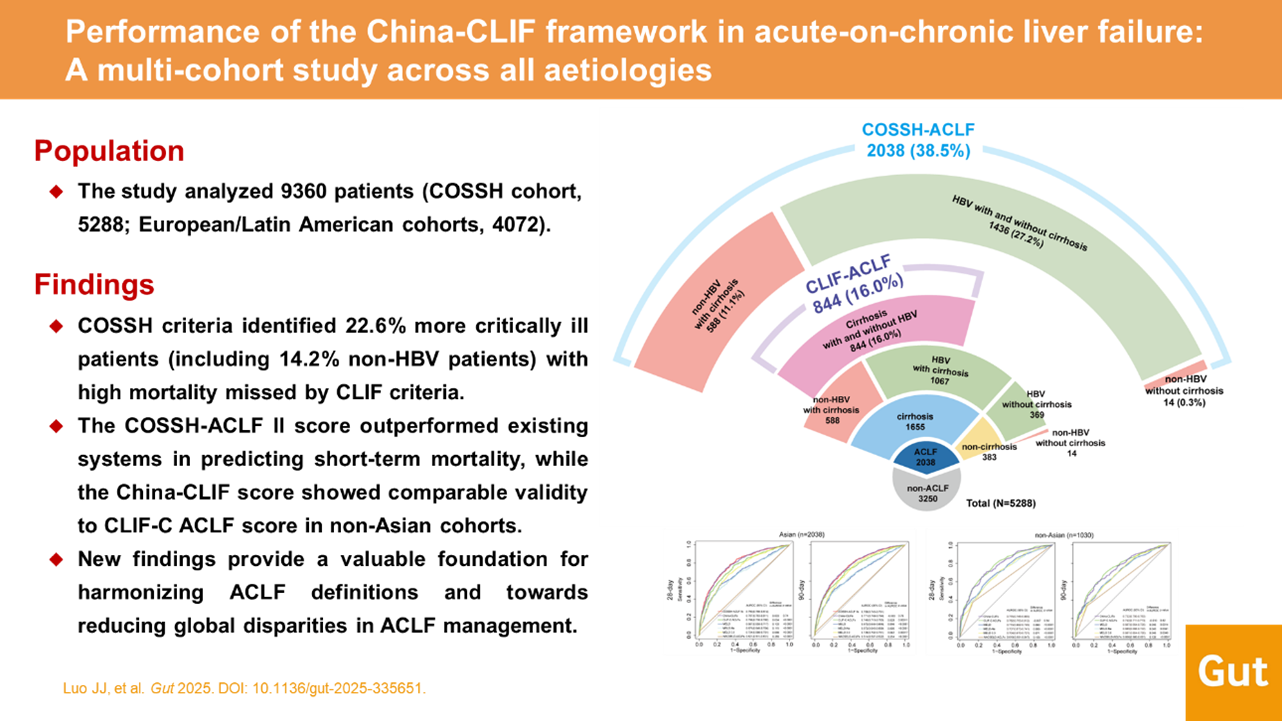
Figure 1. Visual Abstract
Sensitivity and specificity are important for easily applicable diagnostic criteria for ACLF of all aetiologies. Compared with European Chronic Liver Failure (CLIF) criteria, COSSH criteria identified an additional 22.6% of patients as ACLF. These additional patients, although exhibiting organ failure and high short-term mortality, were not captured by CLIF criteria. The study also highlighted limitations of the CLIF definition, which yielded an unbalanced distribution of ACLF severity—over half of patients were classified as ACLF-2 regardless of aetiology. By contrast, COSSH criteria revealed a more epidemiologically reasonable pyramid-shaped distribution across severity grades. This is valuable in resource-limited settings, where accurate risk stratification is essential for prioritizing interventions such as liver transplantation. The study further showed that Asian Pacific Association for the Study of the Liver (APASL) criteria missed patients with extremely high mortality, as it focuses on acute hepatotropic insults and excludes those with prior decompensation. Patients identified solely by APASL criteria had a <15% 28-day LT-free mortality rate, underscoring its limitations compared with COSSH criteria. These results suggest that COSSH criteria better capture high-risk patients, including those with liver-specific injury or extrahepatic insults, who may benefit from timely intensive management.
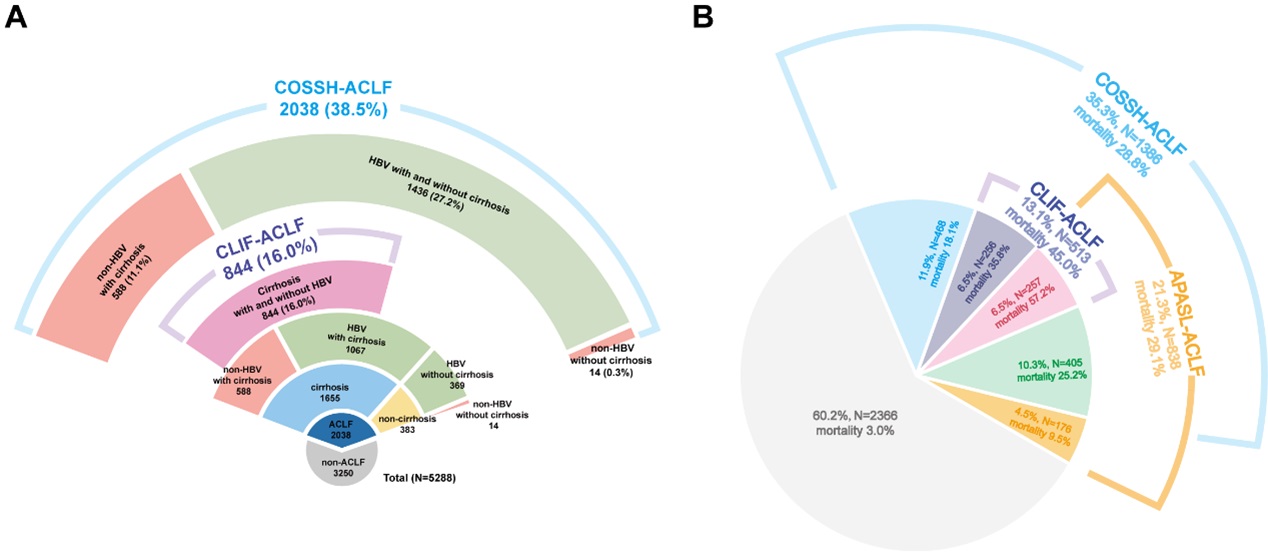
Figure 2. Fan-shaped diagram of diagnostic performance of the CLIF, COSSH and APASL criteria.
A simple and accurate prognostic score is crucial for making informed clinical decisions. The analysis revealed that the COSSH-ACLF II score achieved prognostic performance equivalent to the China-CLIF score in predicting 28- and 90-day LT-free mortality, and both outperformed other scoring systems. This advantage extended beyond patients meeting COSSH criteria to those meeting CLIF criteria, whether HBV- or non-HBV-related. Risk stratification using COSSH-ACLF II score effectively categorized patients into three distinct mortality risk groups. Validation in the CANONIC, PREDICT, and ACLARA cohorts confirmed the robustness of the China-CLIF score in non-HBV populations. A mimic validation of COSSH-ACLF II score, using organ failure frequency data from CANONIC, further supported its predictive superiority. Together, these findings establish the China-CLIF score as a globally validated tool, bridging Asian and non-Asian populations. COSSH-ACLF II score, as a simplified version, shows strong potential for routine clinical implementation.
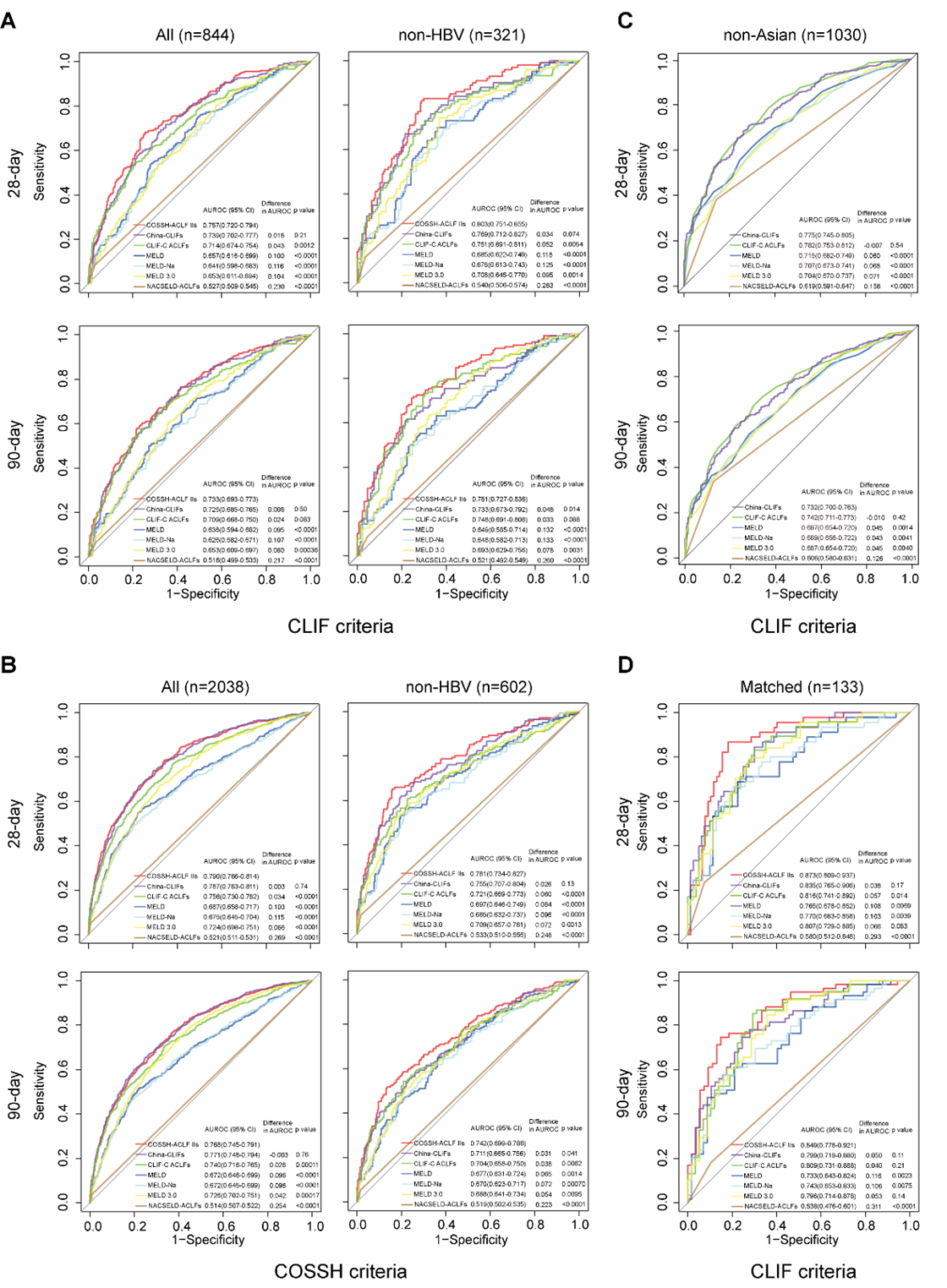
Figure 3. Receiver operating characteristic (ROC) curves for prognostic performance of seven scores at 28 and 90 days under CLIF and COSSH criteria.
In summary, the China-CLIF framework represents a major step toward harmonizing ACLF definitions worldwide by demonstrating robust applicability across diverse aetiologies and regions. Its adoption could help reduce disparities in ACLF diagnosis and management and accelerate the development of effective therapies for this life-threatening condition.
More information: This study was conducted by the COSSH team in collaboration with the CANONIC, PREDICT, and ACLARA Study Groups. Ph.D. candidates LUO Jinjin and HU Meiqian, Dr. FENG Tingting, ZHANG Yliyuan, HUANG Yan, HUANG Yuxian, YE Feng and LI Jiang are the co-first authors of this article. Prof. LI Jun, Richard Moreau, JIANG Jing, Jonel Trebicka, Alberto Queiroz Farias, CHEN Xin, YOU Shaoli, CHEN Yu, LIN Bingliang, Rajiv Jalan and Paolo Angeli are the co-corresponding authors of this article.